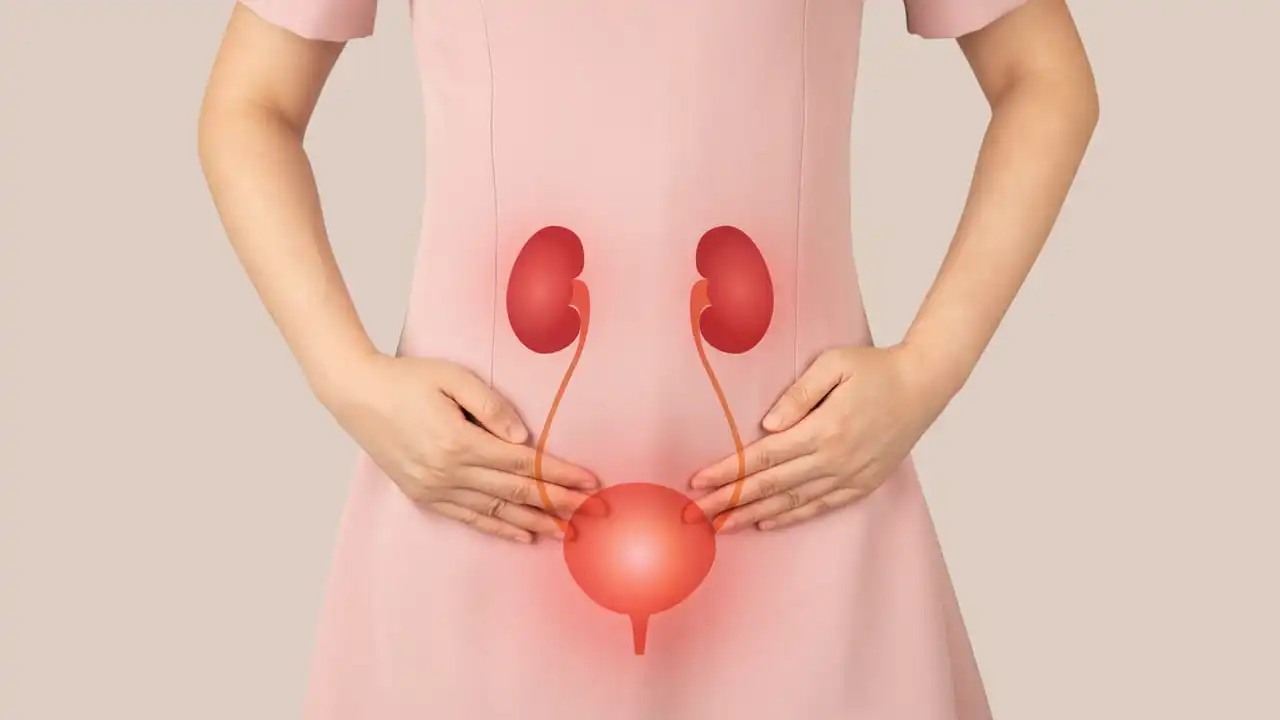
Understanding Urinary Retention: Causes, Signs, and What to Do
Urinary retention means you can't empty your bladder fully or at all. It can be sudden and painful (acute) or build up slowly over weeks to months (chronic). Either way, it needs attention—left untreated it can cause infections, bladder damage, or kidney problems.
Common causes include enlarged prostate in men, urinary tract infections, certain medications (like antihistamines, antidepressants, opioids), nerve problems from diabetes or spinal injury, and pelvic surgery. Women may get retention from pelvic organ prolapse or scarring after surgery. Sometimes the cause is temporary—constipation, alcohol, or anesthesia after surgery.
Spot the signs early
If you feel a sudden strong urge to urinate but can't, or if you strain and only pass a few drops, that's a red flag. Other signs: lower belly pain, a firm full bladder you can feel, weak urine stream, leaking small amounts (overflow incontinence), or repeated urinary infections. With chronic retention you may only notice frequent urination at night, weak stream, or a feeling of incomplete emptying.
Quick steps you can take now
If you can't pass urine and have severe pain, go to the emergency room—acute retention is an emergency. In hospitals they often relieve the bladder with a catheter right away. For less severe cases, try sitting in a warm bath for a few minutes, relax your pelvic muscles, and try to urinate again. Avoid drinking large amounts of fluid quickly and skip alcohol and caffeine until evaluated.
Diagnosis usually includes a bladder scan or ultrasound to measure residual urine, a urine test to check for infection, and review of medications and medical history. Your doctor may order blood tests and more imaging if a blockage or nerve problem is suspected.
Treatment depends on cause. If the issue is a blocked prostate, medications called alpha-blockers (tamsulosin) can help, and sometimes surgery is needed. Infections get antibiotics. If nerves are involved, addressing the underlying nerve condition and using intermittent self-catheterization can control symptoms. For temporary retention after surgery, short-term catheter use is common.
Some drugs target the problem directly. For non‑obstructive retention doctors sometimes try bethanechol to stimulate the bladder. For prostate-related retention, 5‑alpha‑reductase inhibitors (finasteride, dutasteride) shrink the gland over months and lower recurrence. Discuss benefits and timelines with your provider.
Self-catheterization teaches you to empty the bladder at home and lowers infection risk compared to long-term indwelling catheters. Pelvic floor therapy and timed voiding schedules help some people with chronic retention. Discuss side effects and options with your clinician; there’s rarely a one-size-fits-all fix.
Prevention tips: keep bowels regular, check prescriptions for drugs that affect urination, limit heavy drinking, and manage diabetes and neurological conditions closely. Men with prostate symptoms should get regular checkups—early treatment cuts the chance of retention.
If you have repeated UTIs, new lower belly pain, or sudden inability to urinate, seek prompt care. Urinary retention can be solved or managed in most cases, but early recognition makes treatment easier and reduces complications. Early action prevents serious problems often.
Bladder infections and urinary retention: What you need to know
Hey, folks. I thought it's high time we had a chat about something real important - bladder infections and urinary retention. These health nuisances can crop up when you least expect it, affecting your daily life. In this article, I'll be unraveling what exactly these conditions are, their causes, and most importantly, how you can prevent them. Stick around for insider tips on maintaining optimal urinary health. Because trust me, understanding is the first step to prevention.
Read MoreLatest Post
-
DPP-4 Inhibitors and Joint Pain: What You Need to Know 14 November 2025
-
-

-

How Atrophic Gastroenteritis Links to Chronic Fatigue Syndrome 22 September 2025
-
