Topical Steroid Potency Chart: How to Choose the Right Strength to Avoid Skin Damage
Topical Steroid Safety Checker
Check Your Steroid Safety
Enter your application details to see if your steroid choice is appropriate for your specific use case.
Using the wrong strength of topical steroid can turn a helpful treatment into a problem. You might think stronger is better - but that’s not true. Too much potency, too long, on the wrong part of your body, and you risk thinning skin, stretch marks, redness, or even permanent damage. The good news? There’s a simple, science-backed way to avoid this: topical steroid potency charts.
What Does Potency Even Mean?
Potency isn’t about how well a steroid works - it’s about how strongly it affects your skin. A superpotent steroid like clobetasol propionate (Temovate) is 100 times stronger than over-the-counter hydrocortisone cream. That doesn’t mean it’s 100 times better. It just means it’s 100 times more likely to cause side effects if misused. The U.S. FDA uses a seven-class system to rate these strengths:- Class I (Superpotent): Clobetasol, halobetasol, diflorasone - used for thick, stubborn plaques like severe psoriasis.
- Class II-III (High to Moderate): Betamethasone, mometasone, triamcinolone - common for eczema flares on the body.
- Class IV-V (Moderate to Low): Hydrocortisone butyrate, fluocinolone - used on sensitive areas like the face or groin.
- Class VI-VII (Least Potent): Over-the-counter hydrocortisone 0.5%-2.5% - safe for mild irritation and kids.
These aren’t random labels. They’re based on real lab tests that measure how much a steroid shrinks blood vessels in the skin - the gold standard for judging strength. A Class I steroid causes 90% vasoconstriction. A Class VII? Maybe 10%.
Why Potency Matters More Than You Think
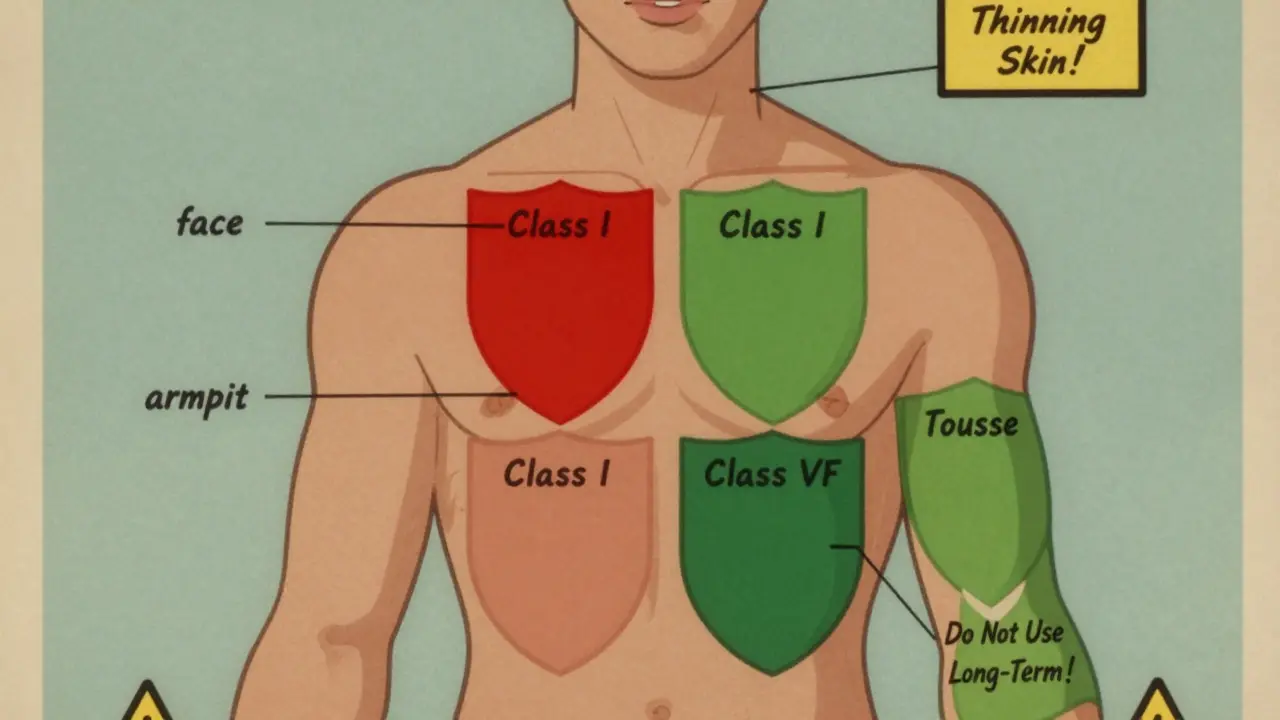
Most people don’t realize that the same steroid can act differently depending on where you put it. Apply a Class IV cream to your face? You’re risking skin thinning. Use it on your elbow? It might be perfect. The Skin Health Institute of Australia found that potency effectively increases by one class when applied to skin folds - armpits, groin, under breasts. That’s because these areas absorb more. Same cream. Different result. Even the base matters. Ointments are greasy, but they lock in moisture and let more steroid get through - up to 20% more than creams. So if you’re using a high-potency ointment on your face, you’re asking for trouble. A cream version of the same drug might be safer.And concentration? Two hydrocortisone creams - one at 1%, one at 2.5% - are in different potency classes. The stronger one is Class VI. The weaker one? Class VII. That’s not a tiny difference. That’s the difference between safe and risky.
Where You Apply It Changes Everything
Your face, eyelids, neck, and genitals have thin skin. They absorb steroids faster. That’s why guidelines are strict:- Face and eyelids: Only use Class VI or VII (like hydrocortisone 1% or 2.5%). Never Class III or higher.
- Armpits, groin, genitals: Class IV or lower. Even Class V can cause thinning if used daily for more than a week.
- Hands, feet, elbows, knees: These areas have thick skin. You can use Class II or III here - but still limit use to 1-2 weeks.
- Large body areas: Avoid high-potency steroids on more than 10% of your skin. Systemic absorption can mess with your hormones.
A 2020 study showed that 42% of patients used moderate-to-high potency steroids on their faces - often because the label didn’t say “do not use on face.” That’s how side effects start.
How Long Is Too Long?
Duration matters as much as strength. The American Academy of Family Physicians says:- Class I steroids: Never use longer than 2-3 weeks.
- Class II-III: Don’t go past 3 months.
- Class IV-VII: Can be used longer - but still, take breaks.
Why? Because steroids suppress your skin’s natural repair system. Use them too long, and your skin forgets how to heal itself. That’s when you get:
- Thinning skin (atrophy)
- Visible blood vessels (telangiectasia)
- Stretch marks
- Acne or rosacea flare-ups
- Topical steroid withdrawal (red, burning skin after stopping)
One in five people who use high-potency steroids for more than 3 weeks develop skin atrophy. And it’s not always reversible.
How Much Should You Use?
Most people use way too much. A single fingertip unit (FTU) - the amount of cream or ointment squeezed from a tube from the crease of your index finger to the tip - covers two adult handprints. That’s it.- One FTU = one adult palm size (front and back)
- Face and neck = 2.5 FTUs
- One arm = 3 FTUs
- One leg = 6 FTUs
Studies show 35% of patients use 2-3 times that amount. That’s not just wasteful - it’s dangerous. More cream doesn’t mean faster healing. It just means more steroid soaking into your skin.
Special Cases: Kids and Chronic Conditions
Children absorb steroids 3-5 times faster than adults. Their skin is thinner, their body weight is lower, and their hormone systems are still developing. That’s why:- Infants and toddlers: Only use Class VI-VII (hydrocortisone 1% max).
- Children under 12: Limit moderate potency (Class IV-V) to 7-14 days max.
- Never use Class I or II on kids unless under direct dermatologist supervision.
One study found 8.7% of children on high-potency steroids developed HPA axis suppression - meaning their body stopped making its own cortisol. That’s serious.
For chronic eczema, doctors now recommend “proactive therapy”: applying a mild steroid (Class VI) twice a week to areas that flare up, even when they look clear. This cuts flares by 68% over 16 weeks, according to the TRAIN study. It’s like preventive maintenance - not waiting for a flare to get worse.
What About Newer Steroids and Alternatives?
Not all steroids are created equal, even within the same class. For example:- Elocon (mometasone) is 25% more potent than Diprosone (betamethasone dipropionate), even though both are Class II.
- Advantan (methylprednisolone) is 30% less potent than Elocon.
And then there are new delivery systems. The FDA approved a hydrocortisone valerate foam in 2021 that delivers 35% more steroid than the old cream - even though the concentration is the same. Potency charts haven’t fully caught up.
That’s why more people are turning to non-steroidal options. Crisaborole (Eucrisa) and ruxolitinib (Opzelura) work well for mild-to-moderate eczema and psoriasis. They don’t cause skin thinning. But they’re slower. A Class I steroid clears 85% of psoriasis plaques in 4 weeks. Ruxolitinib? 72%. So sometimes, you need the steroid - just not for long.
How to Use the Chart Right
Here’s your simple checklist:- Check the label. Is it Class I-VII? If not, ask your pharmacist.
- Match strength to location. Face? Use only mild. Body? Maybe moderate.
- Use the fingertip unit. One FTU per two handprints. No more.
- Set a timer. If you’re on Class II or higher, set a phone alert for 14 days. Stop unless told otherwise.
- Watch for warning signs. Thinning skin, redness after stopping, shiny patches? Talk to your doctor.
Most dermatologists and pharmacies now have digital potency charts built into their systems. If yours doesn’t, download the National Psoriasis Foundation’s free chart. It’s updated for 2025 and includes comparisons to non-steroidal options.
What to Do If You’ve Already Damaged Your Skin
If you’ve used a strong steroid too long and now your skin is thin, red, or burning:- Stop the steroid immediately - but don’t quit cold turkey. Taper slowly under medical supervision.
- Use fragrance-free moisturizers daily. Ceramide creams help rebuild your skin barrier.
- Avoid heat, harsh soaps, and scrubbing.
- See a dermatologist. They can prescribe non-steroidal anti-inflammatories or light therapy to help recovery.
Recovery takes months. But it’s possible. The key? Never go back to the same high-potency steroid without a plan.
Bottom Line
Topical steroids are powerful tools - but they’re not candy. Their strength isn’t a badge of honor. It’s a warning. The right potency, applied correctly, for the right amount of time, can heal your skin. The wrong one? It can break it.Use the potency chart. Know your class. Respect the limits. Your skin will thank you.
Can I use a high-potency steroid on my face if I dilute it with moisturizer?
No. Diluting doesn’t make it safe. Even diluted, the steroid’s molecular structure still affects your skin the same way. You risk thinning, redness, and rebound flares. Always use a product labeled for facial use - Class VI or VII only.
Is hydrocortisone 2.5% stronger than 1%?
Yes. Hydrocortisone 2.5% is Class VI. Hydrocortisone 1% is Class VII. That means 2.5% is about twice as potent. Don’t assume OTC means safe - higher concentration = higher risk, especially on sensitive skin.
Why do some doctors prescribe steroid creams for months?
They shouldn’t - unless it’s a low-potency steroid (Class VI-VII) and they’re using a proactive maintenance plan. For moderate or high-potency steroids, guidelines limit use to 2-12 weeks. Long-term use increases side effect risk. If your doctor prescribes a Class III or higher for months, ask for a second opinion.
Can topical steroids cause weight gain or mood changes?
Yes - but only with very long-term, high-dose use on large areas. Superpotent steroids (Class I) applied over 20% of your body for more than 3 weeks can suppress your adrenal glands and cause systemic effects like weight gain, fatigue, or mood swings. This is rare but serious. Always use the lowest strength for the shortest time.
What’s the safest steroid for babies?
Hydrocortisone 0.5%-1% (Class VII) is the only steroid generally considered safe for infants. Use it sparingly - no more than once daily, for no longer than 7 days. Avoid ointments on diaper areas - they trap moisture and increase absorption. Always check with your pediatrician first.






15 Comments
Branden Temew
December 31, 2025 at 12:34
So let me get this straight - we’re giving people a chart that tells them not to use a nuclear bomb on their face... but somehow people still do it? 😅 I mean, if you put clobetasol on your eyelids, you’re not treating eczema - you’re auditioning for a horror movie. Skin atrophy doesn’t come with a warning label. It just shows up one day like your ex after a breakup: silent, permanent, and weirdly shiny.
Also, why do we still have OTC steroids at 2.5%? That’s not ‘mild,’ that’s ‘I didn’t read the fine print and now my face looks like a balloon.’
Stewart Smith
January 2, 2026 at 05:44
Been there. Used a Class III cream on my neck for ‘just a few days’ to calm a rash. Three months later, my skin looked like tissue paper. Now I use ceramide cream like it’s holy water. And I check the class on every tube like it’s a serial number. Turns out, ‘doctor recommended’ doesn’t mean ‘safe for your face.’
Also, FTUs? I had no idea. I was using half a tube per arm. Oops.
Retha Dungga
January 3, 2026 at 07:06
Yessss 🌿✨ this is the info no one tells you!! I used hydrocortisone 2.5% on my lips bc it ‘felt better’ and now my skin is… different. Like, emotionally different. 🫠 But now I’m all about that ceramide life 💆♀️💛 #skinawareness
Jenny Salmingo
January 3, 2026 at 08:07
I’m so glad someone made this. My mom used steroid cream on my face when I was little. I didn’t know why my skin looked weird until I was 25. Now I tell everyone: don’t use strong stuff on your face. Simple. No need to overthink it.
Aaron Bales
January 4, 2026 at 22:27
Class I = 2 weeks max. Class II-III = 12 weeks max. Class IV-VII = use with caution but no panic. FTU = one squeeze per two handprints. Face = Class VI or VII only. That’s it. No fluff. Follow this and you won’t break your skin.
Brandon Boyd
January 6, 2026 at 09:53
Listen - your skin is not a battery you can overcharge. You wouldn’t run your phone on 100% charge 24/7, so why treat your skin like it’s disposable? Proactive therapy with mild steroids? Genius. It’s like brushing your teeth before you get a cavity. Prevention > damage control.
And yes - diluting doesn’t help. It’s like putting water in your gas tank and thinking you’ll save money. Nope. You just wreck the engine slower.
Frank SSS
January 8, 2026 at 07:00
Okay but let’s be real - most people don’t even know what a ‘fingertip unit’ is. And pharmacies? They’ll sell you Class III cream next to the lip balm like it’s a snack. Meanwhile, your 8-year-old is using it on their cheeks because ‘it stopped the itch.’
And don’t get me started on TikTok dermatologists who say ‘just use it until it’s gone.’ Bro, that’s not a treatment plan. That’s a time bomb.
Paul Huppert
January 8, 2026 at 15:48
Really appreciate this breakdown. I always assumed stronger = faster results. Never realized the absorption differences between ointments and creams. I’ve been using ointment on my face for months thinking it was ‘more effective.’ Oops.
Also, the 42% stat on facial misuse? That’s wild. I’m gonna print this chart and tape it to my medicine cabinet.
Hanna Spittel
January 8, 2026 at 17:31
THEY’RE HIDING THIS FROM US!!! 🤯 Why does the FDA allow Class II on shelves? Who’s approving this? Is Big Pharma paying off the dermatologists? I read a study once that said steroids are linked to adrenal fatigue AND depression. Coincidence? I think not. 🧠💀 #steroidconspiracy
Kayla Kliphardt
January 9, 2026 at 11:51
This is so helpful. I’ve been using hydrocortisone 1% on my hands for eczema and didn’t realize it was Class VII. I was worried I wasn’t doing enough - now I know I was actually being careful. Thank you for the clarity.
John Chapman
January 9, 2026 at 22:44
YES YES YES!! I’ve been telling people this for years!! 😤 You think you’re healing your skin but you’re just making it weaker. I used clobetasol on my arms for a month - now I have stretch marks that look like lightning bolts. Don’t be me. Use the chart. Use the FTU. STOP BEING LAZY.
Also, non-steroid options? Try Eucrisa. It’s expensive but your skin will thank you. No more red, shiny, paper-thin skin. 🙏
Urvi Patel
January 11, 2026 at 15:59
Who needs charts when you have tradition? In my village we used cow dung and turmeric for everything. Now you give us a 7-class system? This is Western overcomplication. Skin heals itself if you just stop touching it. Stop poisoning yourself with chemicals.
anggit marga
January 11, 2026 at 19:49
Why are you listening to American doctors? In Nigeria we use neem oil and shea butter - no steroids needed. This whole chart is a scam to sell more cream. Your skin is not weak - you’re just scared of natural healing. #AfricaKnowsBest
Joy Nickles
January 11, 2026 at 22:31
Wait - so if I use a Class IV cream on my groin for 10 days, I’m risking atrophy? But I’ve been doing it for 3 years?? I just thought it was ‘normal’??? 😭 I’ve been using 3 FTUs every time?? I thought that’s what the bottle meant?? My skin is… I don’t even know what to say… I need to go cry in the bathroom now. 😵💫
Emma Hooper
January 12, 2026 at 00:07
Okay, I’m gonna be real - I used to think steroid creams were magic fairy dust. Now I know they’re more like a slow-acting poison wrapped in a pretty tube. I used to slather on mometasone like it was body butter. Now I’m the girl who brings her own ceramide cream to the beach. My skin looks like it’s been through a war… but at least it’s still attached.
Also - I just bought a tiny measuring spoon. I’m measuring my FTUs like I’m baking a cake. Because apparently, I’m not a grown-up until I know how much cream to use.